Coronary Artery Disease
 |
| Coronary Artery Disease |
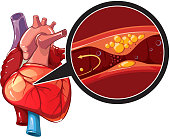
Coronary Artery Disease (CAD) is a condition in which plaques(a fatty deposit on an artery wall in atherosclerosis ) build up in the walls of the coronary arteries (the vessels that supply blood to the heart muscle). These deposits can gradually block the artery, or they can suddenly rupture, causing a more acute obstruction.
Basically, the heart muscle requires a continuous supply of oxygen and nutrients to survive, obstruction of a coronary artery rapidly leads to significant problems.
CAD is caused by atherosclerosis(a disease of the arteries characterized by the deposition of plaques of fatty material on their inner walls),a chronic, progressive disorder of the arteries in which deposits of cholesterol, calcium, and abnormal cells (that is, plaques) build up on the inner lining of the arteries.
Atherosclerosis – the left artery shows a normal lumen (the central cavity of a tubular or other hollow structure in an organism or cell), the right artery illustrates what happens to the lumen when plaques form in the arterial wall.
These plaques can cause a gradual but progressive narrowing of the artery, and as a result, blood flow through the artery becomes more difficult. When the obstruction becomes large enough, the patient may experience angina*.
Angina* refers to the symptoms a patient experiences any time the heart muscle is not getting enough blood flow through the coronary arteries. Angina is usually felt as a discomfort (often a pressure-like pain) in or around the chest, shoulders, neck or arms.
Stable Angina* is angina that occurs, with exertion or after a big meal. Stable angina generally means that a plaque has become large enough to produce a partial obstruction of a coronary artery.
Normally,when a person with stable angina is at rest, the partially blocked artery is able to meet the needs of the heart muscle. But when that person exercises, (or has some other stress that makes the heart work harder), the obstruction prevents insufficient increase in blood flow to the heart muscle, and angina occurs. So stable angina usually means that there is a significant plaque in a coronary artery that is partially obstructing the flow of blood.
In addition to causing obstruction by a gradual increase in their size, plaques are also subject to sudden rupture(see diagram below), which can produce a very sudden obstruction. The medical conditions caused by the rupture of a plaque are referred to as Acute Coronary Syndrome (ACS).
ACS is always a medical emergency.
Unstable angina or Rest Angina – is one type of ACS. Unstable angina happens when a plaque has partially ruptured(see diagram above), causing a sudden worsening of the blockage in the artery. In contrast to stable angina, symptoms in unstable angina occur unpredictably, (that is, they are not particularly related to exertion or stress), and notably, tend to happen at rest.
Patients with unstable angina are at high risk of developing a total occlusion(the blockage or closing of a blood vessel or hollow organ) of the coronary artery, leading to a myocardial infarction(destruction of heart tissue resulting from obstruction of the blood supply to the heart muscle).
Myocardial infarction, or heart attack, is a more dire form of ACS. Here, the ruptured plaque causes a total (or near total) occlusion of the coronary artery, till the heart muscle supplied by that artery dies. A heart attack, therefore, is death of heart muscle.
The seriousness of a myocardial infarction depend largely on how much heart muscle has died. A mild heart attack is one in which only a small portion of the heart muscle dies. A severe heart attack is one in which a large portion of heart muscle dies.
If a patient receives medical attention within a few hours of the onset of a heart attack, the size of the heart attack can be greatly reduced by administering clot-busting drugs, or by performing an immediate angioplasty (surgical repair or unblocking of a blood vessel, esp. a coronary artery) to open up the blocked artery.
Although survived a heart attack, the patient is still at risk. Subsequent heart attacks are possible if more plaques are present in the coronary arteries. Also, depending on the amount of heart muscle that has been damaged, the patient can develop heart failure.
Furthermore, damaged heart muscle can cause a permanent instability in the heart’s electrical system, which can lead to sudden cardiac arrest. So after a heart attack, all of these risks need to be carefully evaluated, and steps need to be taken to reduce each of these risks to the greatest extent possible.
Best way to deal with coronary artery disease, of course, is to prevent it. All of us should do everything we can to reduce our CAD risk factors.
People who already have CAD, reducing these same risk factors becomes even more important, in order to slow the progression of the disease. In addition, several avenues are available for treating CAD, including drug therapy, surgical therapy, and angioplasty and stenting (a stent is an artificial ‘tube’ inserted into a natural passage/conduit in the body to prevent, or counteract, a disease-induced, localized flow constriction).
The treatment of Coronary Artery Disease always needs to be individualized, and optimal therapy depends on careful consideration of all the options, by both the doctor and the patient to prevent an heart attack.

Comments
Post a Comment